Borrelia burgdorferi - Lyme disease
Lyme borreliosis is caused by bacteria. It is the most common tick-borne disease in Switzerland. A common sign of Lyme disease is a certain kind of rash termed erythema migrans. The infection can be treated with antibiotics, but cannot be prevented by vaccination.
Pathogen

Lyme borreliosis is caused by different bacterial species of the genus Borrelia, grouped into the Borrelia burgdorferi sensu lato complex. Six out of more than 20 described species of this complex are known to be pathogenic to humans: B. afzelii, B. garinii, B. bavariensis, B. burgdorferi sensu stricto, B. mayoni and B. spielmanii. For the species B. valaisiana, B. lusitaniae and B. bissettiae, pathogenicity is currently under discussion.
Epidemiology
Lyme borreliosis is widespread in the northern hemisphere (North America, Europe and Asia). Except for B. mayonii, all species pathogenic to humans are found in Europe. Lyme borreliosis is by far the most common tick-borne disease in Europe.
The main vector for the transmission of Borrelia burgdorferi sensu lato in Switzerland is Ixodes ricinus. As opposed to tick-borne encephalitis, the circulation of B. burgdorferi sensu lato is not restricted to natural foci, meaning that the entire range and distribution of I. ricinus ticks (the whole of Switzerland except for altitudes above 1’500 m.a.s.l.) is considered a risk area for infections with B. burgdorferi sensu lato. Pathogen prevalence in ticks is variable, ranging from about 5 % to 30 %, in some places up to 50 %.
Each species of the Borrelia burgdorferi sensu lato complex shows a preference for specific host animals; accordingly, the eco-epidemiology of Lyme disease is highly complex. The density and composition of the host animal population are key factors in maintaining the circulation of B. burgdorferi sensu lato in an ecosystem. Various small mammals, medium-sized mammals, birds, and reptiles have been identified as reservoir hosts.
Lyme disease is not notifiable in Switzerland, therefore the exact incident rate of the disease is not known. However, acute cases of Lyme disease can be reported via the Sentinella reporting system. Since 2008, between 5’300 and 16’800 physician visits due to Lyme disease have been extrapolated in the period from January to the end of September
Clinical manifestation
A high proportion of infections with B. burgdorferi sensu lato does not result in symptomatic disease. The probability of manifesting with Lyme disease after a tick bite is about 1 – 5 %. The risk increases with the duration of tick feeding on its host: prior to 12 – 16 h, the risk is extremely low, but it increases if the blood meal has started longer than 24 – 48 h ago.
The natural course of an untreated infection is highly variable. A disease does not result from every infection. In symptomatic diseases, each type of manifestation can basically occur isolated, but also in different combinations. Lyme disease is a multisystem disease that manifests predominantly as a localized skin infection (erythema migrans). Within days to weeks, dissemination of the bacteria to other organs, most commonly the central nervous system, joints, or myocardium, may occur. Clinical pictures are classified into early localized, early disseminated, and late disseminated stages. Early manifestations of Lyme disease are most commonly observed from spring to fall, according to tick activity; late manifestations of Lyme disease do not have a typical seasonal prevalence.
Early localized stage
An erythematous papule or macule develops at the site of the tick bite after an average of one week. Over days to weeks, an anular lesion develops, often with central healing, which slowly expands and is referred to as erythema migrans. The erythema migrans can be pronounced, but also rather discrete – the manifestations are diverse. Erythema migrans is the most common early manifestation and leading symptom of Lyme disease. The lesion is typically painless, but may be accompanied by burning and itching in rare cases. Erythema migrans may be accompanied by flu-like general symptoms.


Early disseminated stage
Although less common in Europe than in the Americas, multiple erythema migrans are also observed in Switzerland.
Within weeks to months after a tick bite, the central nervous system may be affected. Early neuroborreliosis is the most common manifestation of the early disseminated stage. The classic triad of Garin-Bujadoux-Bannwarth syndrome, consisting of septic meningitis, painful neuroradiculitis, and cranial nerve loss, is observed in only a small proportion of affected individuals.
During meningitis, headaches are prominent; fever, meningismus, nausea, and vomiting are rare. Radiculitis is initially characterized by radicular pain; additional neurologic deficits may follow within a few weeks. Asymmetric motor deficits, which may be accompanied by sensory deficits, are characteristic. Among cranial nerve deficits, the facial nerve is most commonly affected in the form of peripheral facial nerve palsy. This may also occur isolated, without affecting the central nervous system.
The early disseminated stage may also manifest with rheumatologic symptoms that occur within months after a tick bite. The affection pattern of Lyme arthritis is typically mono- or oligoarticular, with the knee joints most commonly affected. It also typically follows an intermittent course, with the number and duration of individual episodes being highly variable.

Carditis is a rare manifestation in Europe and predominantly affects men. Carditis is clinically characterized by arrhythmias – mainly in the form of atrioventricular (AV) blockages of varying degrees; the symptoms are often accompanied by other manifestations of Lyme borreliosis.
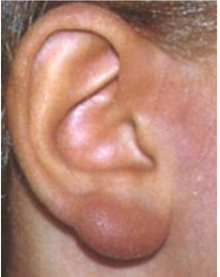
A special type of skin reaction is the Borrelia lymphocytoma (reddish-livid tumor at typical locations such as earlobes, nipples, nostrils or scrotum).
Carditis is a rare manifestation in Europe and predominantly affects men. Carditis is clinically characterized by arrhythmias – mainly in the form of atrioventricular (AV) blockages of varying degrees; the symptoms are often accompanied by other manifestations of Lyme borreliosis.
A special type of skin reaction is the Borrelia lymphocytoma (reddish-livid tumor at typical locations such as earlobes, nipples, nostrils or scrotum).
Picture: Gilbert Greub
Late disseminated stage
During the course of untreated Lyme disease, joint infestation can rarely progress to chronic Lyme arthritis after months to years.
Acrodermatitis chronica atrophicans (ACA) may develop months to years after a tick bite. Patients with ACA experience an initial infiltrative stage followed by the characteristic changes of the atrophic stage: cigarette-paper-thin, wrinkled skin, livid discoloration, and plastic protrusion of vessels. In some cases this is observed together with neurological symptoms of the peripheral nervous system.
A very rare manifestation of the late disseminated stage is chronic neuroborreliosis. This usually develops within a few years after a tick bite. Clinical manifestations include progressive encephalomyelitis (especially para- and tetraparesis) or chronic axonal polyneuropathy.
Therapy
Patients appropriately treated with antibiotics in the early stages of Lyme disease usually recover quickly and completely. Antibiotics commonly used for oral treatment include doxycycline or amoxicillin. We refer to the guidelines of the Swiss Society of Infectiology.
Vaccination
A monovalent vaccine (LYMERix®) is licensed in the USA, but has not been offered since 2002 for commercial reasons. For Europe, neither active nor passive immunizations are currently available. However, clinical trials with new vaccines are ongoing. Pfizer and Valneva have jointly developed a vaccine candidate that is currently being tested. It is a multivalent protein subunit vaccine that targets the “Outer Surface Protein A” (OspA) of Borrelia. This vaccine is intended to provide protection against North American and European species/strains of B. burgdorferi sensu lato.
The company “Mass Biologics” of the University of Massachusetts Medical School has developed a human monoclonal antibody, which is to be used as a pre-exposure prophylaxis for Lyme disease. Clinical trials are expected to begin soon. This approach would provide seasonal protection against Lyme disease. It would likely consist of a single shot that people would receive each year at the beginning of tick season.

Diagnostics

Serology is considered the tool of choice to support clinical diagnosis. Seroconversion occurs 3 – 5 weeks after infection for IgM and 6 – 8 weeks for IgG. Although IgM antibodies are usually detectable earlier than IgG antibodies, cases of erythema migrans and neuroborreliosis without IgM- have also been observed with positive IgG antibody detection. In late manifestations, IgG antibodies are usually detectable, and a negative IgG result is highly unlikely to indicate the presence of a late manifestation. A positive serology only proves a contact with Borrelia and does not allow any conclusion as to whether the disease is active or not. Over time, antibody titers often hardly change and IgM antibodies can remain positive for decades.
Tests should always be performed as a two-step diagnostic. The ELISA is recommended as the first step, the immunoblot or immunodot must only be used in the second step.
An intrathecal synthesis of Borrelia-specific antibodies can be detected or ruled out by assessing the CSF-serum index. This method has a very high significance for the diagnosis of neuroborreliosis. In contrast, the mere detection of antibodies in the CSF is not conclusive, since antibodies detectable in the CSF may also originate from the patient’s serum (i.e., may be passively transmitted). Especially in cases of short disease duration, the intrathecal immune response may be detectable prior to the serum immune response.
Detection of the chemokine CXCL-13 is used to aid in neuroborreliosis diagnosis. Its detection can succeed in the CSF even before the appearance of antibodies. The threshold for a positive result has not yet been officially defined.
Direct pathogen detection by polymerase chain reaction PCR has variable performance depending on the stage of the disease and the type of specimen. The examination of skin biopsies in the case of erythema migrans or acrodermatitis chronica atrophicans as well as the examination of synovial samples in the case of Lyme arthritis has a sensitivity of about 50 – 70 %. Direct detection of Borrelia in cerebrospinal fluid samples in acute Lyme disease cases is about 10 – 30 %. Testing of blood, urine, or ticks is not recommended. Cultural detection is only offered in specialized laboratories and is of secondary importance in everyday diagnostic practice.
All methods mentioned for molecular biological, cultural and serological detection are available at the CNRT.
Guidelines
- Lyme disease Part 1: epidemiology and diagnosis. Rev Med Suisse. 2006 Apr 5;2(60):919-24
- Lyme disease Part 2: clinic and treatment. Rev Med Suisse. 2006 Apr 5;2(60):925-8, 930-4
- Lyme disease Part 3: prevention, pregnancy, immunodeficient state, post-Lyme disease syndrome. Rev Med Suisse. 2006 Apr 5;2(60):935-6, 938-40
- To test or not to test? Laboratory support for the diagnosis of Lyme borreliosis: a position paper of ESGBOR, the ESCMID study group for Lyme borreliosis. Clin Microbiol Infect. 2018 Feb;24(2):118-124
- Review of European and American guidelines for the diagnosis of Lyme borreliosis. Med Mal Infect. 2019 Mar;49(2):121-132
Sources
- National reference center for Borrelia, Germany
- Robert Koch Institute, guide on Lyme Borreliosis
- Federal Office for Public Health FOPH Switzerland, Information on borreliosis / Lyme disease
- Evison J et.al. Abklärungen und Therapie der Lyme Borreliose bei Erwachsenen und Kindern. Empfehlungen der Schweizerischen Gesellschaft für Infektiologie. Schweizerische Ärztezeitung 2005;86: Nr.42
- Gern L et.al. European Reservoir Hosts of Borrelia burgdorferi sensu lato,Zentralblatt für Bakteriologie,Volume 287, Issue 3,1998,Pages 196-204
- https://www.zecken.de
- https://zecken-stich.ch