Babesia spp.
Babesiosis is caused by parasites, which, like the pathogens that cause malaria, can infect the red blood cells. It is particularly present in the north-eastern part of the United States, where the pathogen Babesia microti is transmitted by the tick species Ixodes scapularis. In Europe, this disease is very rare; in Switzerland, no case has been documented so far.
Pathogen
Various species of the genus Babesia can be detected in ticks. Babesia spp. are parasites of blood cells belonging to the order Piroplasmida. In ticks, they undergo a sexual and asexual reproductive cycle; in vertebrate hosts, asexual reproduction occurs after transmission with the ticks’ saliva at the end of a blood meal. Babesia spp. are transmitted both transstadially and transovarially in ticks; thus, ticks remain carriers of the pathogen from generation to generation and therewith serve as a reservoir host for Babesia spp.
The most important Babesia species are pathogens of domestic and farm animals, such as Babesia divergens and Babesia bovis in cattle, Babesia caballi in horses, and Babesia canis in dogs. Other species are more common in wild animals, such as Babesia microti in rodents.
Ticks that carry Babesia spp. in Europe are Ixodes ricinus, Rhipicephalus sanguineus, and Dermacentor spp.
.
Epidemiology
Human babesiosis was first documented in 1956. In Europe, infections with Babesia divergens have been described, but these are rare. They affect splenectomized patients in particular and have a severe, often fatal course. Babesia divergens is responsible for the majority of Babesiosis cases in humans and can also infect immunocompetent individuals. Since 2003, another zoonotic species, Babesia venatorum, has been observed very sporadically in Europe.
In the northeastern United States, infections with Babesia microti are most widespread; the CDC reports about 2000 relevant cases annually. In contrast, babesiosis in Europe has remained exceptionally rare since the first documented case in Germany in 2007, probably due to the low pathogenicity of this species in Europe.
Clinical manifestation
Infections of varying severity are observed mainly in immunocompromised individuals. Infections with B. divergens particularly affect splenectomized patients. However, babesiosis also occurs in immunocompetent individuals, most commonly infections with B. microti in the United States. However, rare cases have also been published in Europe. Clinically, babesiosis manifests with flu-like symptoms, fever, splenomegaly, and hemolytic anemia. Symptoms are similar to malaria (without tropical travel).
Both severe, fatal courses and asymptomatic infections have been described. Because of its uncommonness, babesiosis can be mistaken for other infectious diseases, typically malaria. Hildebrand et.al have even described a confusion with neuroborreliosis.
Therapy
Therapeutic options range from classical treatment of piroplasmosis to combination therapies that include classical antibiotics against bacteria.
Vaccination
There is no vaccine to protect against the disease.
Diagnostics
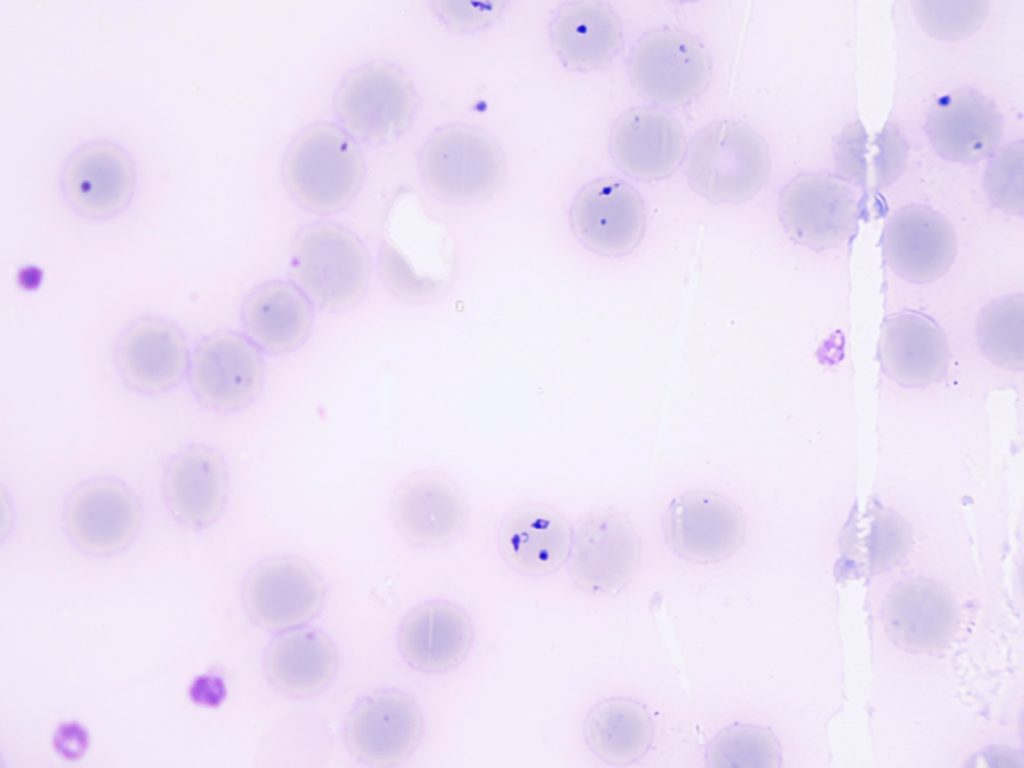
The classical method is direct microscopic detection of the parasites in the erythrocytes in a blood smear and a thick drop stained with Giemsa. This method does not differ from the one used for the detection of plasmodia in suspected malaria. It is the method of choice in the acute phase of babesiosis.
A PCR is available at ADMED Microbiologie to confirm microscopic detection or to increase the sensitivity of detection. It also allows the detection of babesia in other tissues.
The serological method validated in our laboratory is only suitable for the detection of infections with B. microti. It is an immunofluorescence-based method that should only be used in cases of suspected babesiosis on return from corresponding endemic areas (USA).
Guidelines
n.d.
Sources
Hildebrandt A, Zintl A, Montero E, Hunfeld KP, Gray J. Human Babesiosis in Europe. Pathogens. 2021 Sep 9;10(9):1165.
Martinot M, Zadeh MM, Hansmann Y, Grawey I, Christmann D, Aguillon S, Jouglin M, Chauvin A, De Briel D. Babesiosis in immunocompetent patients, Europe. Emerg Infect Dis. 2011 Jan;17(1):114-6.